This series on BBC’s “Transgender Kids: Who Knows Best?” is co-authored by HJ Hornbeck and Siobhan O’Leary. It attempts to fact-check and explore the documentary’s many claims concerning gender variant youth. You can follow the rest of the series here:
- Part One: You got Autism in my Gender Dysphoria!
- Part Two: Say it with me now…
- Part Three: My old friend, eighty percent
- Part Four: Dirty Sexy Brains
Eighty percent is tired. Eighty percent has had thrust upon its back the concern trolling of every clueless media pundit from Sarah Ditum to Jesse Singal. And the exterminationists, the “transsexuals will sort themselves out later” types, they too abuse my poor poor friend eighty percent. Eighty percent is the one and only quote the antagonists will reliably provide. Eighty percent is the crux of hundreds of thousands of very, very concerned words printed in very, very concerned columns.
Eighty percent is just exhausted, being expected to carry all this.
Eighty percent deserves a rest.
Recall from part two:
“Transgender activists don’t like the high rate desistance to be talked about because if you know that 80% of gender dysphoric children are going to end up as ordinary gay men, I’m going to encourage all of them to adapt to their anatomical sex and the handful that are destined to be transsexual no matter what will sort themselves out later.”
–Ray Blanchard
Gather ’round, kids, and join me for an episode of street magic, wherein I break down step by step the flick of the wrist and the sleight of hand dearest Ray Blanchard has engaged in for the past, oh, 40 years. Just as the magician lies when he says he has performed magic rather than dexterity and misdirection–so, too, does Ray Blanchard.
If I were to give a tutorial on a card trick or something similar to that nature, I suppose I would begin by waxing philosophical on the guiding principles of “magic”–that is, directing the audience to focus on one thing whilst performing some otherwise obvious act of deception with the other. So too shall I begin with lofty principles, with the specifics to come in a moment.
Imagine for a moment you’ve suffered from a terrible car crash. You’ve suffered a great many number of injuries of variable severity and will perish without the skillful intervention of a trauma surgeon.
Now imagine you are given the opportunity to choose between two surgeons. One of them says, “We’re going to prioritize your breathing and your circulation while we assess the damage. We’ll suture up any ruptured veins and arteries, we’ll patch your organs back together, we’ll wire all your bones back together and throw everything in a cast. We’ll connect you with an outpatient clinic to nurse your physical and mental health back to normal, or as close as we can get.”
The other says, “ah, well, I fixed up a guy from a bar fight once, so I’ll make it up as I go along. You’ll sort yourself out later.”
I imagine the choice would be rather obvious, and I likewise imagine you’d be hard pressed to find someone who seriously objects to giving you the opportunity to benefit from a health program rather than expecting you to roll the dice.
I’m curious, then, why pundits line up around the block to lecture trans people when we’ve made our choice. Now that Blanchard has admitted to believing what we’ve said he’s believed since the 70s, perhaps I can naively hope it has become obvious to outsiders why quote-un-quote “trans activists” are so adamant about the former CAMH Sexologists. Blanchard has violated the magician’s creed, see, “a magician never gives up his secrets.” It’s not exactly he-said-she-said anymore, is it? Blanchard said it point blank: His secret is that He Doesn’t. Fucking. Care.
We can finally sidestep the issue of the fact that nearly all of Zucker’s and Blanchard’s former patients have been saying this entire god damn time and focus on the fact that Blanchard has fully and unapologetically disclosed that his true intentions have never at any point pretended to give the single tiniest dust-specked iota of a fuck about the health and well-being of trans people.
Because now you get it. Now you know not just what we’ve been saying. You know why we’ve been saying it. You wouldn’t trust the nonchalant trauma surgeon to patch your life together, so why the fuck would we?
We wouldn’t. But the system didn’t give us a choice. Blanchard was our healthcare, for years. Zucker was our healthcare until 2015.
Just think about that for a moment, and maybe it becomes obvious why so much of our activism has painted a target on psychiatry. Maybe, suddenly, all that “shouting” comes into focus.
the handful that are destined to be transsexual no matter what will sort themselves out later
the handful that are destined to be transsexual no matter what will sort themselves out later
the handful that are destined to be transsexual no matter what will sort themselves out later
The story goes, according to Zucker et al. and the never-ending concern trolls lining up around the block to write about trans kids, is that 80% of the children admitted for “gender dysphoria” related care “desist,” that is, stop experiencing dysphoria, by the time they mature. Thus the logic is to then assume most children are in fact cisgender and would suffer under any transition related services they may be “mistakenly” entered in to, along with some scaremongering through some painfully predictable vocabulary: “irreversible,” “permanent,” “regret.” Usually at this point they do a mental backflip straight on to surgery*, because castration anxiety is–pardon my French–a bitch. If you learn nothing else from this series, please just remember to be extremely suspicious of anyone who leaps from “children” to “surgery.” Nobody practicing under the Worldwide Professional Association of Transgender Health is advocating or performing surgery on endosex children. Once again I will reiterate that it is only intersex children who are subjected to harmful and unnecessary surgery, so if the pearls of castration anxiety must be clutched, you will kindly direct them there where they are actually needed.
Contrary to Blanchard’s claim that “trans activists” don’t like 80% desistance to be “talked about,” I’ve compiled a list of nearly every trans feminist I know and–surprise!–we’ve all talked about it.
- Zinnia Jones
- Brynn Tannehill
- Sam Hope
- Mercedes Allen
- Monica Roberts
- Kelley Winters
- Cristan Williams
- Julia Serano
- Me
Can I just say that if the plan is to keep “80% desistance” under wraps that trans feminists are doing a fabulously bad job at it?
Of course, what Blanchard means is separate from what he says. What Blanchard means when he says we don’t “like talking about it,” is “we get impatient the same way actual scientists get impatient with Flat Earther conspiracy theorists.” None of those articles is an obsequious admission of defeat. “Oh yeah, 80%, you got me, haha, you’re right.” That’s because the statistic in question: is 1) factually dubious; and 2) what remains after clearing the clutter is irrelevant under gender affirmative models. What Blanchard means is that “trans activists” don’t roll over and accept the wisdom of a discredited crank who still has no shortage of trans-suspicious pundits throwing themselves at his feet and kissing the toe of his shoe.
So now that we’ve discussed the flourish designed to bring our attention away from the act of deception, let us look at the sleight of hand.
The year is 1978. The Diagnostic and Statistical Manual of Mental Disorders (DSM) is in the workings of its third iteration following the declassification of homosexuality as a mental illness. The term “transsexualism” is replaced with “gender identity disorder in childhood” (GID) under a class of illnesses deemed “psychosexual.”** Despite the fact that Dr. Robert Spitzer’s work is used to declassify homosexuality as an illness, the stigma merely shifts to the new GID diagnosis on the basis of the exact same body of work.
Cristan Williams, quoting The Making of the DSM-3, notes that the DSM-3 GID workgroup succeeded in its efforts to remove this body of work and create an early diagnostic distinction between embodied dysphoria–the primary element of DSM-3’s GID–and dissatisfaction with gender role, not deemed a disorder. (emphasis mine)
A major concern is that the category tries, but fails, to differentiate true identity confusion with failure to follow sex stereotyped roles… Such a failure is unforgivable and unacceptable. There is a real philosophic argument on how to impart gender identity without imparting sexual stereotypes [but] it does become imperative … that in these criteria we must remove all sex-stereotyped material.
…
If one compares the Gender Identity Disorder of Childhood section in the April 15, 1977 draft of DSM-III with the section in the revised draft of January 15, 1978, it is readily apparent that almost the entire category had been reworked with an attempt to meet the concerns of Chappell and the other critics. In the later draft, under “Essential Features” and “Diagnostic Criteria:’ the discussions of boys and girls were done separately. The new descriptions were written so as to stress the significant pathology of the disorder, and they explicitly declared, “There is not merely the rejection of stereotypical sex role behavior as, for example, in ‘tomboyishness’ in girls or ‘sissyish’ behavior in boys.”
To make it clear in plain English: The DSM-3 work group made a distinction between nonconformity with respect to gender roles and the anxiety embodied because of sexed attributes. Under these diagnostic criteria, a GID diagnosis maps much more closely to a particular trans experience–one which typically responds well to Hormone Replacement Therapy and sometimes Gender Reassignment Surgery. But the key thing to note is that people other than the crusty, old, white, cishet men understood that gender nonconforming behaviour in children was not the same thing as anxiety produced from one’s subjective experience of one’s sexed attributes. The transgender children admitted to these programs would be the sliver of intersecting circles in this DSM-3 work group diagram (dysphoric children who could not, or would not express nonconformity were unlikely to present for care at this time).
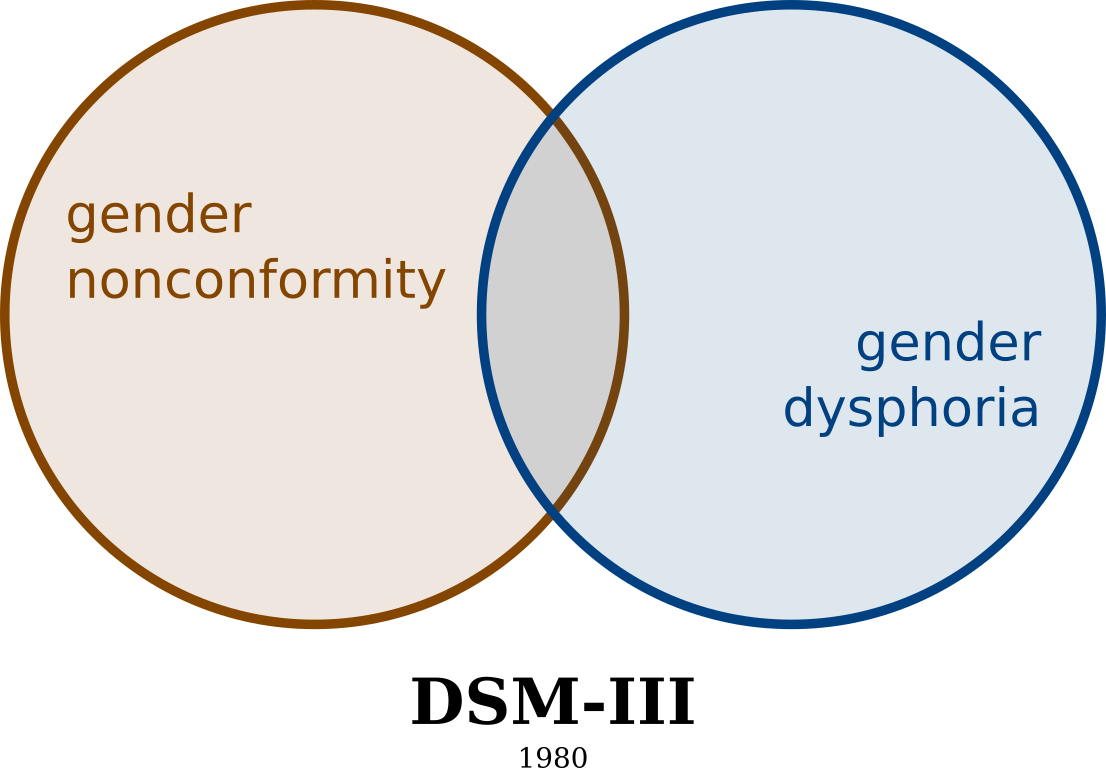
“Gender Identity Disorder” in the DSM-3 work group.
Guess who was on the GID workgroup for the DSM-4? Kenneth Zucker and Ray Blanchard.
Imagine my surprise when the crusty bats that had predicated their careers on Sissy Boy Syndrome aversion methodologies suddenly saw an opportunity to revive their practice as long as they claimed to cure trans kids rather than gay ones.
Again, it should be noted that after CAMH sexologists became part of the Gender Identity Disorder Workgroup, the distinction between the embodied gender dysphoric and gender role nonconforming experience was purposefully removed.
Here’s the part where my card trick tutorial shows that the card has been secretly pocketed during an act of sleight of hand: If the diagnostic criteria for GID were changed such that anxiety caused by sexed attributes (“gender dysphoria”) was no longer distinguishable between dissatisfaction with a gender role (“nonconforming behaviour”), then the GID diagnosis was being applied to children without regard to whether their needs about their body would change as they matured.
Having erased the distinction, the DSM-4 then claims all children with GID are “transgender” and that “gender dysphoria” “resolves spontaneously” most (80%) of the time.
Illustrated, this asserts that gender dysphoria and dissatisfaction with gender role are interchangeable. Thus anyone who complains about the utter imprisonment that is gender roles can be called “trans.”
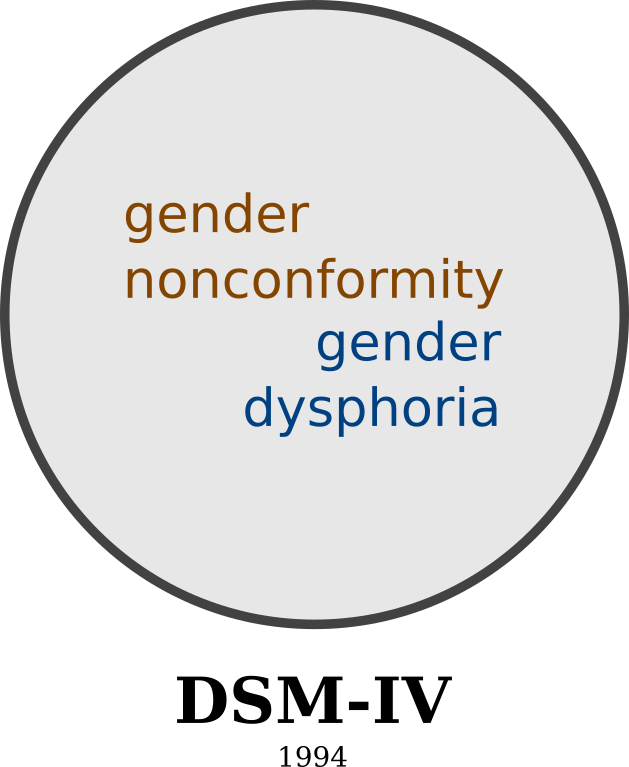
“Gender Identity Disorder” in the DSM 4.
Which now means we can finally roll around to our 80%-shaped cudgel.
Having erased the distinction between gender role and gender identity, Dr. Zucker & co. can now claim that all their patients are “trans” as children. But early feminists*** validated the experiences of trans folk by understanding our experience was not merely one of expectations of society (the gender role) but also of a complex relationship with our body. Without the distinction, non-transgender (i.e. cisgender) children who called poppycock on gender roles were considered the same as children experiencing anxiety from their sexed attributes. Then the children who were mostly dissatisfied with gender roles, not experiencing anxiety with their sexed attributes, did not grow up to pursue Hormone Replacement Therapy or any kind of transition-related surgery, which Zucker & co. claimed meant they ceased believing they were trans.
Thus, the methodology that you can force “trans kids” to “adopt to their anatomical sex” was born. It wasn’t that 80% of transgender children “desisted”****, it was that 80% of children entered into this kind of system never would have needed to transition.
Now recall HJ Hornbeck’s observation from p1: (emphasis mine)
If there was a correlation between autism and dysphoria, we’d expect it to be consistent across child- and adulthood. But if I was able to show there’s no evidence for a correlation in adults, then how can there be a strong correlation in childhood? That can only happen if a) either autism or gender dysphoria are not persistent, contrary to how they are defined, or b) one or both conditions are being overdiagnosed in children. Given that children are adults that haven’t fully baked, it should not be a surprise that their behaviors can vary substantially more than adults. This makes it easy to over-diagnose one condition or the other, artificially inflating the correlation.
Just to reiterate: This is not “hiding” from the 80% talking point. This is putting the information out there in plain sight. Folks would rightly be pissed off if something like chemotherapy were being prescribed for a head cold, but for some reason trans people are expected to accept this sledgehammer from our doctors.*****
Special thanks to HJ for the pretty Venn diagrams.
-Shiv
*See below:
Their genitals and “the surgery” which, let’s not kid ourselves, to cis people there is only ever one surgery and that is bottom-surgery. It’s fucking everywhere.
…
To them, that’s all we become. And our humanity is subsumed into that automatic trigger. And this happens to the point where writers writing about us from a position of bias can’t stop flicking their tongue against that wound as they write, freaking out about the poor penii and uterii of the world and lamenting the idea of a cis person ever going through the horror we regularly expect trans folks to go through.
**Insistence on the use of the term “transsexualism” indicates at best the speaker/writer is a whopping 30 years behind the times. Insistence on the use of the term “gender identity disorder,” as Sarah Ditum so often does, is likewise an indication of arbitrary support for finally-discredited 90s psychosexual nonsense.
***The stereotype of the transphobic “Second Wave” is a bit unfair. Even many transphobic second wave feminists recanted their position eventually, such as Gloria Steinam; others were always trans inclusive and were surprised their works were being misapprehended to justify transphobia, like Catherine MacKinnon, Judith Butler, and Andrea Dworkin.
****Can we just take a moment to appreciate how fucked up this term is? “Desist” is something lawyers and cops tell you to do when you’re breaking the law.
*****The DSM-3 work group may have de-stigmatized gender nonconforming behaviour but the final version that was published promptly paved over it. It’s also worth noting that the actual GID diagnosis would’ve been stigmatizing either way.