I weighed 7 pounds, 7 ounces when I was born on Saturday, 9 March 1957, at 7:07 in the morning. I know this because all the 7s were memorable, but mainly because this is what doctors and nurses do: they document everything.
You know this. Everytime we visit a doctor, they write down our weight, our height, our blood pressure, every parameter they can squeeze out of us. I can go online right now and read the doctor’s notes on every medical visit I’ve made in the last 20-some years — every prescription, every measurement, all of my complaints, every recommendation, every vaccination…it’s all there. Doctors are obsessive record keepers. There is so much medical data stored away that I sometimes wonder how anyone can extract useful information from it.
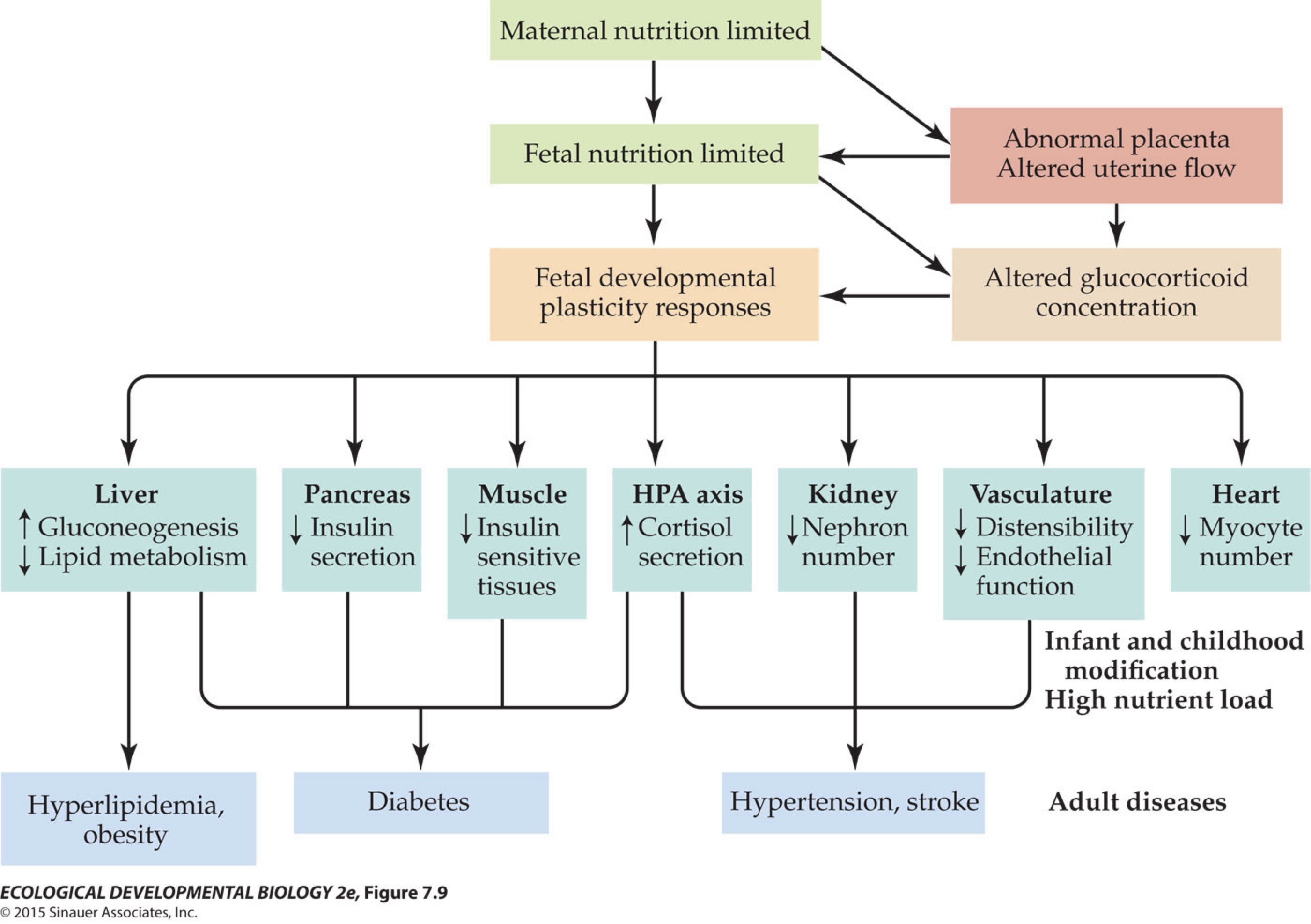
But they have! One attempt that has had significant influence was to correlate birth weight data in infants with their adult history of cardiovascular disease. Surprise, your weight on the day you were born is associated with your blood pressure, 60 years later (in a broad statistical sense, of course — this is a population-level correlation.) This led David Barker to make the specific hypothesis that “poor nutrition, health and development among girls and young women is the origin of high death rates from cardiovascular disease in the next generation.” This idea has since been broadened to form the developmental origin of adult disease hypothesis, that all kinds of medical phenomena have their origns in fetal development, and in the environmental effects that have influenced that development.
Credit where credit is due, the original exploration of the hypothesis was thanks to careful records kept by one midwife, Margaret Burnside, who assisted in the birth of over 15,000 babies in Hertfordshire between 1911 and 1930, and also the records of over 2000 births at Jessop Hospital in Sheffield between 1907 and 1924. They then compared birth records with death certificates in the 1950s-1990s to extract the first hints of associations.*
There’s a huge industry of papers being turned out now that look at correlations between birth weight and adult medical conditions. We’re also seeing more complex connections between disease and growth rate in the first year.
Some of them are very well established associations with low birth weight, like hypertension, coronary artery disease, non-insulin dependent diabetes, stroke, dislipidaemia, elevated clotting factors, and impaired neurodevelopment. Other ‘problems’ have been associated with low birth weight in a small number of studies — there really are amazing numbers of papers where researchers mine the medical data for connections, some of them possibly spurious. So small babies may be more likely to develop issues with chronic lung disease, depression, schizophrenia, and general behavioral problems. They may have reduced uterine and ovarian size and precocious pubarche. They might be more prone to breast and testicular cancer.
Surprisingly, they may also marry later, if at all, be left-handed, and have denser fingerprint whorls. You can find it all in the scientific literature.
If you are thinking that you were a plump, fat baby, so you have nothing to worry about, think again. There are correlations between large birth weight and breast cancer (everything seems to cause breast cancer,) prostate cancer, childhood leukemia, and polycystic ovary disease.
This week in my eco devo course, we talked about this hypothesis, and I also handed out a bunch of papers, a different one for each student (there are so many papers in this field!), and today we’re going to have the students assess the literature. It should be fun! The goal is to get a feel for how strong or how valid the various correlations actually are. We’ve also discussed the Dutch famine data. The Nazis starved much of Holland, including the major cities of Rotterdam, Amsterdam, and Leiden, for 7 months in 1945, until the country was liberated by the Allies.
Wasn’t that nice of Nazis to do a massive experiment on a whole nation of 9 million people for us? They let women in each trimester of their pregnancy subsist on 580 calories/day, and then went away and let us analyze the effects. Maternal malnutrition in the third trimester turns out to be bad for babies, who knew? Anyway, the subtext for this week, as it should be for every week, is that Nazis are bad***.
The bigger message is, of course, that development matters and has lifelong consequences, and good, responsible governments provide adequate nutrition to pregnant women and children.
*All these records were handwritten on pieces of paper! The effort to transcribe everything and extract the information in a computational form must have been daunting.**
**My daughter is currently involved in a research project to use natural language processing to synthesize information stored in modern medical records at UW Madison Department of Medicine. That’s useful for a lot of reasons, including drilling down through years of impenetrable treatment notes.
***I hope that overtly political message doesn’t get me in trouble with the university administration.

I weighed 9 pounds and 2 ounces when I was born, at 0844 on 16 July 1964. My mum was a nurse, so she was used to remembering details like this. When I was old enough to understand, she made sure that I knew this information, and that while she knew that I had a good, healthy birthweight, she personally wished that I’d been a little smaller and had popped out an hour or two sooner!
Pathetically, one of the groups deeply afflicted by the Nazis is duplicating and inflicting the same experiment today on a different population. We don’t need more of this data, ever. Then there are other third world conflicts preventing adequate pre and post-natal nutrition in Sudan and the US.
Twins tend to be smaller – does this mean twins are more likely to have certain problems?
One problem with medical data is that the medical corporations are very conscious of the dollar value of their data and refuse to share it with anyone not acting for the companies’ financial interests. This means studies that might show that a medication is not useful or that a cheaper form or type of treatment is better can be suppressed.
Are you going to discuss how genetics can affect these theories?
My babies were all in the healthy 6.5 lb. to 7.5 lb.range, but 4 out of the 5 have autoimmune issues.
Those autoimmune diseases are present in both my husband and myself, as well as people in our family trees going back a few generations.
IIRC, the increased risk of schizophrenia during the Dutch famine was linked to malnutrition in the first trimester and maybe the second, but not in women in the third trimester (i.e. births early in the famine). Lots of other problems in third trimester starvation though. Ezra Susser’s work was particularly important in showing this.
I’m glad that there is more research in adult outcomes of preterm/low birthweight/malnutrition despite the greater difficulty of conducting such studies. There was much interest a couple of decades ago in infant outcomes such as bronchopulmonary dysplasia, cerebral palsy, retinopathy etc., but little grant support for long term studies.
@5–
The difficulty with this research is teasing out all the possible effects. In the Dutch WW2 baby cohort, was the increase in schizophrenia due to malnutrition during the pregnancy, malnutrition during early childhood, the severe cold and other privations of the ‘Hongerwinter’ of 1944/45, or the social trauma of living under Nazi occupation?
We know that the most profound effects were in those who experienced famine during early gestation, but the research also provides some surprising outcomes, e.g. ‘The effects of famine were independent of size at birth, which suggests that programming may occur without altering size at birth.’
Another weird bit of medical history from the Dutch famine: paediatician Dr Willem Dicke noticed that children in hospital with coeliac disease got better when flour was unavailable, and relapsed almost immediately when food restrictions eased and they were served bread. This lead to the gluten hypothesis, and the life-saving development of gluten-free diets.
Famine after birth delays delays the diversification of the commensal bacteria in the gut, which in turn has an effect on development apart from the malnutrition itself. It is amazing humans are robust enough to survive childhood with so many things that can go wrong.
.
About breast cancer. This may sound counter-intuitive but some men get it too. Apparently the vulnerable tissue type appears in both men and women (but in different amounts).
With so many kinds of cancers I would like to emulate the elephants and whales and have lots of extra copies of anticancer genes.
#4: This course focuses on environmental factors, so we don’t delve into the genetics much.
#6: Yes. The consensus of my class after reading several papers on the developmental origin of adult diseases is that they were mostly unconvinced. Too many variables! In particular, most of the subjects were stuck at the same socioeconomic status from birth to old age, so how do you isolate all the factors? You can’t.
Some of the papers looked like p-hacking: they did correlations with a whole slew of variables, and the one that came out statistically significant gets named in the title.