Everyone and their mother is sending me this story today: C-sections May Be Changing the Course of Evolution.
Rates of caesarean section are increasing in countries like the U.S. and the U.K. and a new study suggests that more and more women need the surgery because of their narrow pelvis size — a trait that evolution would, in theory, have weeded out.
For the paper, published in the journal Proceedings of the National Academy of Sciences, researchers used data from the World Health Organization and other large birth studies and determined that cases where the baby is too big for the birth canal — a.k.a. obstructed birth — have increased from about 30 per 1,000 in the 1960 to 36 per 1,000 today.
I say the paper doesn’t show a causal relationship.
Has the rise in C-sections affected human evolution? This scientist predicts yes.
Human ingenuity increasingly allows us to fight back against “natural selection” and, in effect, influence the path of our own evolution.
Take Cesarean sections, the procedure in which babies are born via surgical incision rather than through the mother’s birth canal. Some form of the procedure has been around for hundreds of years, but only in the past few decades has it become commonplace.
In the US, C-sections now account for 30 percent of all births, according to the Centers for Disease Control and Prevention. But back in 1970, that figure was around 5 percent. So while C-sections have only been widely available to mothers for just a couple of generations, already scientists are speculating that the procedure is affecting human evolution.
This scientist says probably not.
The paper itself argues for obstetric selection in humans.
Compared with other primates, human childbirth is difficult because the fetus is large relative to the maternal pelvic canal. It is a long-standing evolutionary puzzle why the pelvis has not evolved to be wider, thus reducing the risk of obstructed labor. We present a mathematical model that explains the high rates of fetopelvic disproportion by the discrepancy between a wide symmetric phenotype distribution and an asymmetric, “cliff-edged” fitness function. Only weak selection for a large newborn, a narrow pelvis, or both is necessary to account for the high incidence of fetopelvic disproportion. Because the regular use of Caesarean sections has reduced maternal mortality, the model predicts an evolutionary response of fetal or maternal dimensions, increasing the rates of fetopelvic disproportion.
Nah, not buying it.
Actually, they do do what they say: they present a mathematical model of how a disparity between head size and pelvic canal size could hypothetically lead to a selection effect, given a particular frequency of disproportion. They don’t actually measure or observe anything, though. They pull together a number of factors, like the heritability of pelvic and head size, and estimates of the frequency of serious birthing difficulties, etc., all of which show a wide range of reported values, and then put together an abstract series of calculations to show that hey, this could potentially have an effect. That’s it. Don’t panic. We’re not looking at an imminent future of bulbous-headed babies and pencil-hipped women because we’ve removed an important constraint on selection.
Without criticizing their calculations, I have to point out that their assumptions (which to their credit they do note) are faulty. You can’t assume from the frequency of Caesarian sections that there is an equivalent frequency of pelvic diameter – fetal head size disparity. C-sections are an extremely indirect measure of that parameter, one that is prone to all kinds of irrelevant noise…I mean, cultural influences.
Here, for instance, is the frequency of c-sections by country.
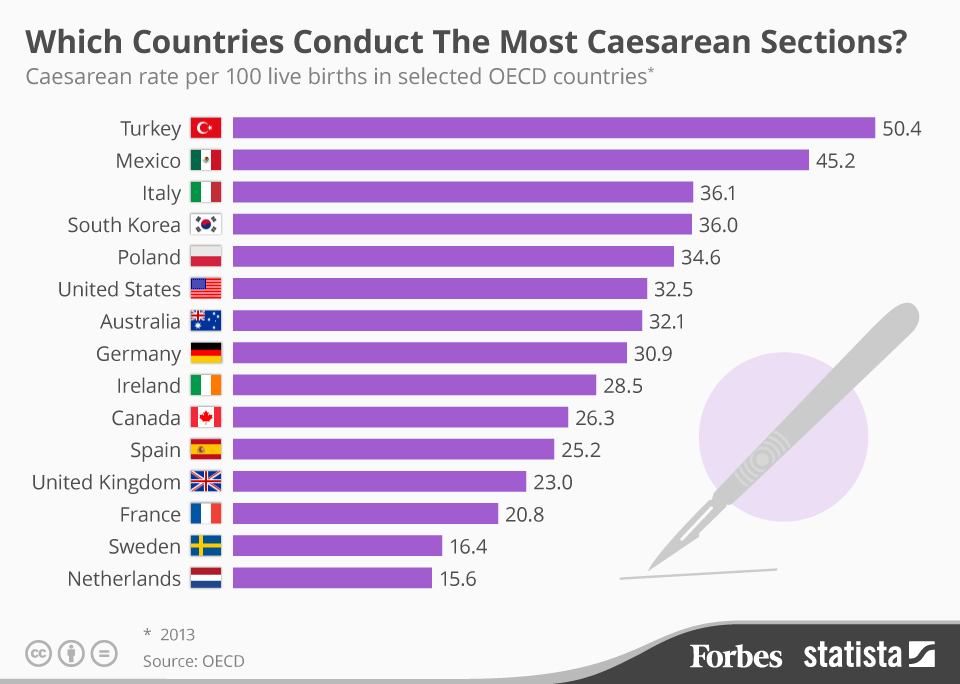
Do you think Turkey and Mexico have huge numbers of giant-skulled babies straining to burst out of their slender-boned mommas? Or that in Sweden and the Netherlands they have more pin-headed babies that slip lightly from their mothers’ gargantuan hips?
Or maybe, just maybe, some significant number of c-sections are unnecessary surgeries, and the differences represent nothing but different biases in medical practice? (However, if your doctor advises that you need one, don’t let this fact dissuade you. You might be one of the people who really, really needs a c-section.)
The World Health Organization has reported that in many countries, c-sections are done at an excessive rate, and that above a certain level, c-sections do not reduce negative effects.
Several studies have shown an inverse association between CS rates and maternal and infant mortality at population level in low income countries where large sectors of the population lack access to basic obstetric care. On the other hand, CS rates above a certain limit have not shown additional benefit for the mother or the baby, and some studies have even shown that high CS rates could be linked to negative consequences in maternal and child heath.
Bearing in mind that in 1985 the World Health Organization (WHO) stated: “There is no justification for any region to have CS rates higher than 10-15%”, we set out to update previous published estimates of CS rates worldwide, and calculate the additional number of CS that would be necessary in those countries with low national rates as well as the number of CS in excess in countries in which CS is overused.
This means that c-section frequency is a really bad proxy for a selection pressure. Note also that the United States’ c-section rate is well above the reasonable frequency. That 25% increase in the rate here probably does not represent any significant change in the degree of selection going on.
The math is nice, but it’s poorly rooted in any real biological phenomenon. Although it turns out that making predictions about evolving babies is a good way to get oodles of press.

Well, that’s disappointing. Given the overwhelming correlation between big heads and super technology, such as FTL, flying saucers, and death rays, I was hopping bigger heads, and thus all those other things, were in our near future.
I don’t know. It doesn’t sound all that unreasonable to me, though the popular news article is obviously flat wrong. They’re claiming a 10-20% increase off of a ~2.3% base prevalance. That may be a large overestimate if they’re assuming most of those 2.3% of cases were due to heritable characters (which wouldn’t be the case for, e.g., underage pregnancies), depending upon their model, which I didn’t look into in too much detail.
But either way, we’re talking about a change from roughly 2.0% to 2.3%, which is barely noticeable in absolute terms and can’t have much of an impact on human populations for many generations. Furthermore, any part of that increase which isn’t due to heritable characters would dilute the spread of any related alleles dramatically.
A couple of things to remember
1. many women have an elective cesarean
2. epidurals increase the frequency of birth interventions such as cesareans
I had an emergency cesarean after 4 hours of pushing. I did have an epidural so that could have contributed. But labor hurts like @#$%%$&^%$!#%^&%, and after 32 hours of labour I couldn’t take it any more and said “give me the epidural now!!!1!!!!!”. Any woman that gave birth without an epidural is my absolute hero!
My daughter’s head was right on the 50th percentile for circumference, so not a giant head. I don’t really have child bearing hips though. If there is a next time they said I should have a cesarean straight away.
I was also born by emergency cesarean. So there may be something to it. However, I am not sure if this is a significant loss of selection pressure on humans compared to all the other things that modern medicine allows people to survive these days.
I’ve always speculated that the invention of spectacles might have led to an increase in vision problems.
I’m pretty sure that if I’d been born in prehistoric times with my profound myopia, I’d have wandered off a cliff long before I reached reproductive age.
Of course, in the event I haven’t reproduced in this era either, so… lousy anecdata I guess.
It does sound plausible on the face of it until the other factors PZ cites are taken into account….and there’s data behind it.
In January 2016, the New York Times printed an article that noted that the key determinant of whether a given birth was cesarean was….wait for it…..the choice of hospital in which the mother elected to give birth. Also, the more informed the patient is, the lower the incidence of c-sections, with physicians having some of the lowest percentages.
http://opinionator.blogs.nytimes.com/2016/01/19/arsdarian-cutting-the-number-of-c-section-births/
The suggestion that incidence of c-sections is related to possible evolutionary change is an interesting speculation, but ultimately unsupported by data.
Surely to goodness there hasn’t been enough time for any kind of medical intervention to have affected human evolution? Much less a surgical procedure that hasn’t been even relatively safe for the mother for more than a couple of hundred years tops?
(fun fact – Julius Caesar’s birth is most definitely not the origin of the word. His mother, Aurelia, gave birth naturally and lived for about forty years after that. There was a theory, which we know from Plutarch, that his family cognomen comes from a distant ancestor of Julius who was born with surgical intervention (from the Latin past participle caesum – having been cut), but it’s actually more likely to come from caesaries – an adjective meaning hairy).
Let’s not forget that size is hardly the only reason for a C-section. Sometimes you just have to get the kid out NOW because something’s gone wrong.
There are other medical reasons for c-section, such “fetal distress” and maternal pre-eclampsia. Also, in certain countries, there are more women giving birth at older ages. I had my child at age 39 so my uterus was not performing well enough to push the baby out. I was more upset that I would have to wait longer to eat and I was really hungry
As I understand it, better nutrition has played a role in average human heights increasing over the centuries. I imagine that birth weights have also gone up because of better nutrition (where available). Attributing changes in the human species to C-sections ignores many other potential contributing factors.
soo. the observation that started this “discussion” is based on something that isn’t even statistically significant?
My understanding of evolution is that *if* c-sections were prevalent, vaginal births would become no longer conserved and can (but not necessarily) atrophy, ja?
Ichthyic@10, you can’t say whether or not the difference is statistically significant just based on those numbers. Statistical significance is jargon with a particular technical meaning; you’d need the standard errors for those two estimates to be able to say whether or not the threshold for statistical significance was reached. I think you might mean to say that the difference isn’t of any appreciable practical significance…?
Didn’t Jack Whatsisname, the guy who founded Codman Research, do this at Dartmouth in the 1970s, in his famous “Small-Area Variations” study, showing that even among 3-digit zipcodes in rural New Hampshire, the rate of C-Sections varied wildly? Almost all due to physician training and preference?
Add to that the rising Me-First-Ness among the Upper Middle Class GenXrs, where now lawyers and consultants and investment bankers routinely schedule C-sections so that their work schedules aren’t inconvenienced, and, as one commenter noted above, superior diagnostic techniques to identify entail problems with a vaginal deliver…..y voila, a few percentage points seems rather devoid of evolutionary portent.
About that WHO 10 -15% “statistic” it actually has no basis in fact –
In 2009, the World Health Organization quietly withdrew the target rate. Buried in its handbook Monitoring Emergency Obstetric Care, you find this:
“Although the WHO has recommended since 1985 that the rate not exceed 10-15 per cent, there is no empirical evidence for an optimum percentage … the optimum rate is unknown …”
Actual analysis of the data showed something else: https://www.ncbi.nlm.nih.gov/pubmed/17302638
“Although very unevenly distributed, 15% of births worldwide occur by CS. Latin America and the Caribbean show the highest rate (29.2%), and Africa shows the lowest (3.5%). In developed countries, the proportion of caesarean births is 21.1% whereas in least developed countries only 2% of deliveries are by CS. The analysis suggests a strong inverse association between CS rates and maternal, infant and neonatal mortality in countries with high mortality levels. There is some suggestion of a direct positive association at lower levels of mortality” (Which in plain English means if you have access to C-section you have a better chance of surviving your delivery and so does the baby)
The optimal C-section rate statistic was apparently made up from whole cloth by Dr Marsden Wagner a pediatrician who served as head of maternal and child health at the WHO. Countries with C-section rates below 10-15% have pretty bad numbers when it comes to maternal and perinatal mortality.
How do we decide which are the “un-necessarians” ? yes some C-sections are performed because there is something that looks concerning on the fetal monitor, so they do a C-section and you have a nice healthy baby. Do we wait and not do C-sections until it’s Really Really an emergency? Until the baby has permanent brain damage due to a compressed cord or Erb’s palsy and a non- functional arm due to shoulder dystocia? Until the woman has gone into convulsions from pre-eclampsia/HELLP syndrome? Until the head becomes trapped during an attempted breech birth.
Yes some of the babies in these situations will be OK if born vaginally, and some won’t die but they will be hurt, possibly permanently. If it’s a C-section or a 1% chance of death and a 4 percent chance of profound brain damage your baby will probably be OK…unless they are the unlucky 1%.
Ok, this is not scientific, but allow me to comment as the mother of five and as a former midwife’s assistant who assisted on 35 births.
First of all, forcing a woman to give birth flat on her back with her legs up in stirrups is the absolute worst position for giving birth possible. This physically narrows the birth canal. If you look at drawings from the past of women giving birth, you see them squatting, kneeling, or using a nifty thing called a birthing stool. This is the natural way to widen the birth canal.
Next, adding medications makes the mother less able to participate in pushing her baby out. If her senses are dulled, she might not be able to recognize the clue that her body is giving her when it is time to push.
Also, I’ve read that many caesarean sections are performed for the convenience of the doctors or the mothers. Personally, I find this to be deplorable. I feel that c-sections should be reserved only for true emergencies.
As for my own experience, I had my first baby in a hospital. There are many reasons that the experience made my husband and I both swear “never again”, barring a real emergency. One of the strongest reasons was the fact that I had to spend so much of my energy during labor fighting off the nurses who tried to persuade, insist upon and finally force me to accept drugs. They would force my husband out of the room to check me and try to force interventions on me while he was out.
She was born naturally, but we were not at all satisfied with that experience.
My other four babies were all born at home. I was free to move around as I wished during labor and to eat as much as I liked.
I was able to choose my own position for giving birth, which for me was kneeling on a blanket next to my bed. Midwives use techniques to help mothers that most medical staffs seem to be unaware of. I definitely did not have to be concerned about fending off offers of drugs. I found giving birth to my babies with no drugs and no interventions to be easy and even pleasant.
I know that there will be immediate condemnation from those of you who consider home birth to be unsafe, but with a well-educated midwife who knows how to spot a complication and when to seek help, it can be safe and much more pleasant for all involved.
I worked for my midwife, and witnessed the experiences of other families, too. I saw mothers who had successful vaginal births after previous c-sections for a “small pelvis” by birthing in a squatting position. It can make a huge difference.
anbheal @13 C-section rates also vary between hospitals because if you are a University teaching hospital you get a lot more of the complex and high risk cases. The bigger hospitals also have the Level 3 and 4 NICU units. If you get the more high risk pregnant patients you also get earlier, smaller, sicker babies. A population of much older or much younger mothers or poor mothers who don’t get pre-natal care, is going to be a population that probably has more complications (obesity or diabetes, or high blood pressure or extremely high or low birth weight – gestational diabetes will give you a BIG baby in some cases.
Some community hospitals and more rural small hospitals don’t necessarily have an anesthesiologist on site 24/7, or they may not have as many. They may choose not to do ANY C-sections. A high rate just means a hospital does more C-sections, it doesn’t tell you why. And if I need a C-section I think I would want someone who has done a lot to do mine. Not the person who last did one years ago.
As to scheduling an induction or C-section – I would have liked the option, I was active duty military married to military and was being transferred 3 months after the birth. Scheduling would have meant being able to have my mother fly in for the birth. Some people have older kids and scheduling would mean being able to get childcare. It doesn’t mean anyone who wants to schedule their delivery is being a “special snowflake”. Please schedule other operations and medical procedures all the time ffs.
magistramarla #15
Why is this deplorable? It is great that you had your choice after your first child. Many women choose an elective caesarean for various reasons. I suggest people condemning your choice for having a home birth is on par with your judgment on others having an elective CS.
I have occasionally wondered why thin-hipped women didn’t all get selected out over 50,000 years ago.
Sometimes I invert that and wonder why big-brained babies survived.
@magistramarla, 15:
I am sorry for your experience in the hospital and glad that you have found the right way for yourself, but please don’t judge. My sister has the exact opposite experience from yours, and horribly so. Her first son died from asphyxiation during a home birth (which, luckily, doesn’t have so much to do with her decision, it would propbably have happened in a hospital too), and since then, she’s had three healthy kids all through c-section. She works with pregnant women, too, and the most important thing is: she let’s them make their own decisions and does not judge them for whatever, but assists them, no matter what they decide.
Midwifes do not possess knowledge that other health professionals don’t, and (myself just now trying to conceive with my partner through IVF and having been warned it might be necessary for her to have a c-section) I would run away from anybody (doctor, midwife or whomever) who claimed some kind of uberspecial knowledge and tried to convince me without being transparent and giving me good reasons to do one or the other. In the end, it surely needs to be the individual decision of the woman, with whom and what she feels comfortable.
The Skeptical OB goes into more detail on this paper and the numerous problems with its assumptions:
http://www.skepticalob.com/2016/12/are-c-sections-changing-the-maternal-pelvis-maybe-but-this-paper-doesnt-show-it.html
@15:
She has an explanation for that, too. From the linked article:
She goes on to argue it’s about positioning of the baby more than size.
Come on white supremacists put a positive spin on this
First rule of evolution is selection, right? Has the rise in C-s significantly reduced child mortality?
I see embraceyourinnercrone has already and in depth addressed that 10-15% nonsense. Thank you for saving my time.
Magistramarla
No, just no.
Can we drop that shit? I happily gave birth to my babies exactly like that. I don’t think I could have squatted anywhere. The best position for giving birth is the one the person doing the pushing feels comfortable in and that is safe.
Because we all know that people in the past had special and accurate medical knowledge. That’s why their outcomes were just so much superior to ours…
There is no scientific data to back that up.
That’s some misogynistic shit right there, denying women pain relief for some supposed (but not really demonstrable) benefit. You know what? I couldn’t get an epidural but hell I wish I could. I remember that I was begging the baby to stop this whole birth thing for 30 seconds so I could breathe.
Why? That’s like saying that many wisdom teeth are extracted as a preventive measure but it should be reserved for true emergencies when’you’re crying in your doctors office with pain.
What’s wrong about a pregnant person deciding that they don’t want to wait and not know when, that they don’t want be pushed into an extreme situation where things pretty much happen beyond people’s control? Why shoukd a person who doesn’t want to go through a vaginal delivery have to? There’s a safe alternative to it and if you recognise a person’s, especially a woman’s right to bodily autonomy then you must recognise her right to choose how to give birth.
+++
Well, C-sections present a bit of an ethical dilemma: A lot of them are done because of a probability. If the risk for a serious adverse outcome without a C-section is 1% then you perform an “unnecessarian” on 99 people but only 1 really benefits from it, but you cannot tell who it is in advance. Maybe you could if you collected more data, but it would be highly unethical to risk that one percent to do so.
+++
Bernardo Soares
Wishing you and your partner the best of luck.
@Gilliel:
Thank you! The whole experience makes me acutely aware of the advances of modern medicine, as well as the efforts of reactionary christian asshats in Poland to ban both women’s access to decent healthcare, abortions and IVF, because if you want a family, you’ll have to get on your fucking knees and pray hard to the big asshole in the sky. It also lets me side-eye the “natural” bullshit even more than before.
Btw, the skeptical OB also links to a study on that “natural” birthing position:
http://www.skepticalob.com/2010/07/oops-upright-birth-positions-increase.html
Really, please. Modern medicine is one big effort to PREVENT NATURAL SELECTION. I would’ve died from asthma as a child. But I had intensive care. Ach! My genes have been passed on. Cruel asthma genes. I would have died from anaphylactic shock from nut allergy–oh–but I had ICU care, ventilator, etc. They saved me. Alas those genes passed on too. I would’ve died from breast cancer due to the BRCA mutation in my family. But they saved me and I reproduced! Maybe I should not have children to prevent my genes from remaining in the population. Oh, and my friend with cystic fibrosis had a baby! What will that do to the gene pool? Production of carriers. Hemophiliacs too. Oh the gene pool! Oh the humanity!
I’ll note that there’s one other factor driving the increase in C-Sections in the U.S., at least: Tort law.
I see a LOT of daytime TV during my lunch break at work, and the commercials during the Maury Povich show are crammed with attorneys offering to sue for a variety of causes. One of the regular pitches is for a child born with any of a number of defects, or mother who suffered any of a source of ailments, with “late or no C-section”. I suspect that in litigious areas, doctors are more likely to perform a C-section because the local courts have decided that active intervention is invariably better than cautious non-intervention (even though it’s always going to be a judgement call).
So the doctor’s malpractice insurer most likely encourages a more strongly interventionist approach.
Even if the premise were true, wouldn’t it only be a viable selection criteria if:
1) The child were female (so only about 50% at best); and
2) the mother AND the baby died in childbirth?
I would think as long as the child survived, the selection, while possible would be minimal.
Giliell @23
Thank you. My first pregnancy ended in labor that was an even bigger nightmare for me for autistic/sensory reasons, with medical staff determined that things needed to progress “naturally” and me being too paralyzed by, well, myself, to fight all their “you want to do right for the baby, right?” with the idea that I might matter, too. Finally there was enough distress on both my part and the baby’s part for — a little ironically — my mother to step in and insist they do something. So, c-section. I’m not going to say that was perfect and painless or anything of the sort, but in many ways it overrode the nightmare preceding it. So much so that two and a half years later, the ob-gyn mentioned a planned c-section in passing, literally glossing over it to rush to the next option glorifying VBAC, and my head shot up and I actually made some sort of eye contact and everything…”Wait, back up, I can do that?!” And we planned it all out that day. Girlchild, of course, had other plans concerning her birth date, but it was still by c-section, at my insistence, even though she came here almost half the size of her brother (and weeks early). I have told people over the years — mostly to their horror — that I would never had had another kid without benefit of a c-section, no matter what. It’s not unnecessary surgery if it is needed to save my sanity.
I’m all for C-sections when necessary, but Amy Tuteur (the “skeptical OB”) is a complete jerk I don’t listen to, pretty much the same way I don’t listen to Richard Dawkins.
“A mother who has feto-pelvic disproportion with an 7 pound baby and requires a C-section could subsequently deliver an 8 pound baby is a successful vaginal birth.”
If it’s due to malpositioning, it’s not feto-pelvic disproportion at all.
It is a significant difference, statistically.
The 95% confidence interval on 30/1000 is +/- 2.8.
You can run a z test for yourself here.
Still a blowhard, I see.
What the hell bullshit is that? You can’t have a confidence interval on a single number.
For a simple model, if we had replacement birth rate in the population, and we suddenly made a deleterious mutation (10% chance of death in childbirth) become neutral, but changed nothing else, how many generations until the formerly-deleterious mutation doubles in prevalence?
@ravensneo
Thank you ! I am not crazy !
I don’t understand what the fuss is all about. It doesn’t seem absurd to me that this would happen, but whether it does or not is irrelevant. If medicine changes the course of evolution, so f***ing what ??? Culture in general does (see lactose tolerance in adults).
Just because something is naturally evolved doesn’t mean it is Good with a capital G. Humanists oppose social darwinism for exactly this reason. We are conscious and empathetic, and our daily choices are often in opposition to natural selection, and that’s a good thing. Sick people, starving people, should be left to die just because that’s natural selection. It is our role as a society to take care of those who need help.
We are not gazelles in the savannah, leaving behind the weeker members of our group to be eaten by predators. We are humans, we take care of each other, and nobody should care if it messes with natural selection.
roachiesmom
It’s sad that there’s so much naturalistic woo-woo about childbirth and child rearing around. I admit that I bought into some of the bullshit myself and the person hurt the most by it was me. I had too vaginal deliveries (no pain relief because my kids really wanted out. I spent about a third of the time typical for first time mothers in the delivery ward for both of them combined). And it later pained me when women who had c-sections thought that their birth was somehow inferior or a failure and that my births were some sort of achievement.
I am completely unconcerned about the rate of c-sections. I am concerned about women and other pregnant people being coerced, lied to, sold woo, ignored and generally not treated like people.
irene
What’S the relevant information in your #29?
We have three sons, all were delivered by C-section. The first was an emergency as after many hours of labor, where his head never entered the birth canal, fetal distress was detected. Even though he was late by two weeks, and dis-mature, he was 8lb 14oz with a head circumference well outside of the normal range The second was scheduled on physicians advice and came out at 10lb 8oz and his head was just as large. Both of them had CAT scans at 11 months old to rule out hydrocephaly as their growth charts showed their heads to be growing outside of normal curves. The second one topped 200% of normal at 11months. That’s when we were told by the pediatrician of category in the diagnostic manual; asymptomatic familial megaencephaly, occurring in 6% of the US population. So when the third son showed up at 11 months with a head that was only 150% of normal no additional tests were run.
I think that C-sections saved my wife’s life and that of our sons, so yes we may be modifying natural selection by saving those who’d otherwise not survive child-birth but so what? I think of it as human directed evolution.
All that being said though I still think that it should be a last resort. From everything I’ve learned recovery from a C-section is much harder and longer than a vaginal birth even if an episiotomy must be performed.
Neither of my children had any such problem – but. When I was almost 3 weeks overdue with the first child, my doctor said we’d have to schedule a C section. I was not really happy about this, but I realised we couldn’t let it go on forever. I suggested induction. He pointed out that the baby was nowhere near the right position for birth and that all an induction would do would be to start a labour which couldn’t progress properly and he’d have to be called out for an emergency section and no one actually wants the emergency version if they can avoid it. So that’s what we did.
I have no idea how many “scheduled for convenience” C sections are actually alternative versions of late pregnancy going not as well as it should, on top of all the cases where mother and/or baby are in serious danger.
I was two weeks late (a pattern I’ve maintained through my life). My mom’s doctor recommended a c-section… and that’s when I decided it was time to come out on my own.
At least, that’s the story I’m told. I have some doubts I was actually able to understand the words at the tender age of not yet born. And I suspect I may have gotten some help from mom and the medical staff.
How does such nonsense even get published? Maybe I’m just one of those mean assholes in my field who wouldn’t take long at all to write back to the editor to say “not worth publishing – not anywhere or ever”. Actually I was much worse with the last such submission that I received and I gave the authors a lengthy review of what was wrong with the submission.