When you’re not grounded by evidence, speculation can take you to some very wild places.The Frontline COVID Critical Care Alliance, or FLCCCA, is one of those quack organizations still pushing ivermectin as a COVID-19 cure. Its founder, Dr. Paul Marik, has been the author on two papers that were retracted, the most recent of which was due to “a series of strong, unsupported claims based on studies with insufficient statistical significance, and at times, without the use of control groups.” More recently, Marik has sued his employer for refusing to allow him to prescribe ivermectin to COVID-19 patients as part of his “MATH+” protocol. He’s actually developed three distinct protocols.
We developed the MATH+ protocol to provide guidance for the treatment of the pulmonary phase of this disease with the goal of reducing the hospital mortality from this devastating disease. However, it soon became obvious that our emphasis needed to shift to the prevention and early (home) treatment of this catastrophic disease to prevent patients progressing to the pulmonary phase and requiring hospitalization (…). Hence, we developed the I–MASK+ and the Test and Treat protocols. […]
And, finally the Post–COVID syndrome or “long–hauler syndrome” has emerged as a common and disabling disorder, and its pathophysiology is poorly understood. We offer the I–RECOVER protocol to help treat this disabling disorder. Recently, the post–vaccination syndrome has emerged as a problematic entity; we believe that the I–RECOVER protocol has utility in treating this syndrome.
The above is taken from the January 1st, 2022 refresh of all three protocols, which you can read here. TwinkBride Pearl on Twitter had a look at the summary of I-MASK+, and spotted something unexpected.
Spironolactone is a little infamous, due to what else it is commonly prescribed for.
Physical interventions should be addressed in the context of adolescent development. Some identity beliefs in adolescents may become firmly held and strongly expressed, giving a false impression of irreversibility. An adolescent’s shift towards gender conformity can occur primarily to please the parents and may not persist or reflect a permanent change in gender dysphoria (…). Physical interventions for adolescents fall into three categories or stages (…):
1. Fully reversible interventions. These involve the use of GnRH analogues to suppress estrogen or testosterone production and consequently delay the physical changes of puberty. Alternative treatment options include progestins (most commonly medroxyprogesterone) or other medications (such as spironolactone) that decrease the effects of androgens secreted by the testicles of adolescents who are not receiving GnRH analogues. Continuous oral contraceptives (or depot medroxyprogesterone) may be used to suppress menses.
That’s right, puberty blockers that improve the health and well-being of transgender youth, and thus are a popular target of TERFs and transphobes, could also help treat COVID. Dig around in the FLCCCA’s FAQ, and you’ll find a link to this paper. Emphasis mine:
These observations combined with our understanding of SARS-CoV-2 molecular mechanism of infectivity lead us to believe that spironolactone is an ideal candidate drug for the prophylactic treatment of SARS-CoV-2. Spironolactone is a safe and well-tolerated anti-hypertensive and anti-androgenic drug used since 1959, that is effective to maintain normal blood levels (…), address heart function, and provide cardio- and renoprotection (…).
While spironolactone is a safe and unexpensive option, it may act in multiple sites against COVID-19 […] Hence, spironolactone meets corresponding epidemiological data, mechanistical plausibility, and sufficient safety profile to become a candidate against COVID-19.
Cadegiani, Flavio A., Carlos G. Wambier, and Andy Goren. “Spironolactone: an anti-androgenic and anti-hypertensive drug that may provide protection against the novel coronavirus (SARS-CoV-2) induced acute respiratory distress syndrome (ARDS) in COVID-19.” Frontiers in medicine 7 (2020): 453.
It isn’t alone, either. A quick search on Google Scholar brings up multiple opinion pieces recommending “Spiro” as a COVID-19 treatment.
The benefits of spironolactone, its extensively validated safety/risk profile, and its ability to substitute for ACEIs/ARBs appropriately would allow this switch without major ethical concerns in selected patients.
Cadegiani, Flávio A. “Can spironolactone be used to prevent COVID-19-induced acute respiratory distress syndrome in patients with hypertension?.” American Journal of Physiology-Endocrinology and Metabolism 318.5 (2020): E587-E588.
Our hypothesis is that spironolactone is the preferred renin–angiotensin–aldosterone system inhibitor to favorably modulate the proteins that determine viral processing and cell entry (…). Indeed, spironolactone has been proposed as a drug to provide protection against COVID-19. .. If proven, this could have an immediate impact because spironolactone is widely available, well tolerated, and inexpensive.
Wilcox, Christopher S., and Bertram Pitt. “Is Spironolactone the Preferred Renin–Angiotensin–Aldosterone Inhibitor for Protection Against COVID-19?.” Journal of Cardiovascular Pharmacology 77.3 (2021): 323-331.
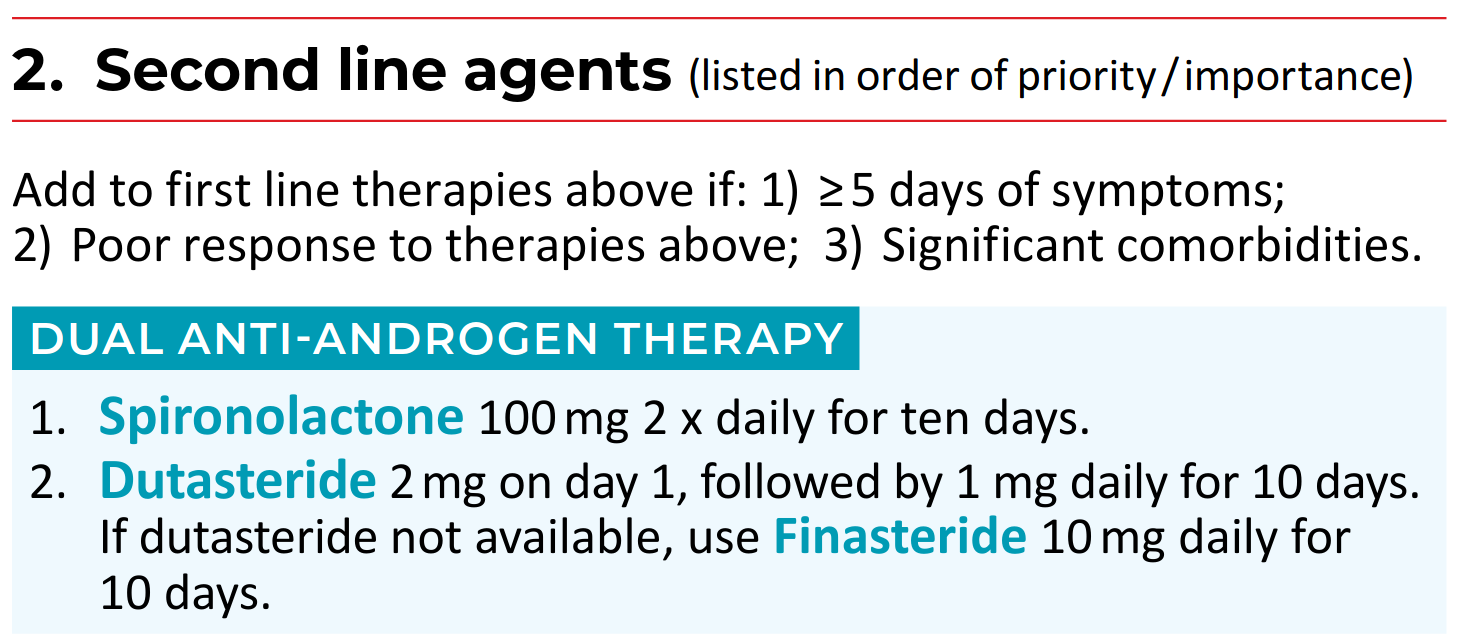
I say “opinion pieces” because, based on my skim of Google Scholar, nobody’s even bothered to run a pilot study. It’s all speculation, at this point. Nonetheless, Paul Marik not only recommends puberty blockers as a second-line therapy for early treatment of COVID-19, his dosage is the same as what’s recommended for transgender women. Alas, his I-MASK+ guidelines only prescribe them for ten days, so it won’t have much effect on a person’s secondary sex characteristics.
17. The Long Haul COVID syndrome (post-COVID syndrome)
… Up to 80% of patients experience prolonged illness after Covid-19. LHCS is not only seen after the COVID infection but it is being observed in some people that have received vaccines (likely due to monocyte activation by the spike protein from the vaccine). LHCS may persist for months after the acute infection and almost half of patients report reduced quality of life.
… A puzzling feature of the LHCS syndrome is that it is not predicted by initial disease severity; post-COVID-19 frequently affects mild-to-moderate cases and younger adults that did not require respiratory support or intensive care. […]In general, while the treatment of ‘Long COVID” should be individualized, the following treatments may have a role in the treatment of this disorder. In addition, the I-RECOVER protocol may have a role in the treatment of post-vaccination syndrome.[…]
Optional: Antiandrogen therapy which results in macrophage repolarization. Spironolactone 50-100 mg BID and dutasteride 1mg daily.
His I-RECOVER guidelines, on the other hand, allow a low dose of Spiro for an indefinite time to a wide swath of the public. I can’t find any place where he bans adolescents from the therapy. While it is again a second-line therapy, if you could tolerate or dispose of the most harmful first line drugs, like ivermectin, you could easily petition to have Spiro added if symptoms persist.
Consider handing this information to a kid from a fundamentalist Christian household, who would have no hope of obtaining puberty blockers if they wanted it for gender-affirming care. This quack just inadvertently gave that kid another pathway to a safe and effective treatment, provided they can tilt the guidelines to their favour.
Wouldn’t it be lovely if COVID-19 inadvertently leads to an uptick in adolescents getting gender-affirming treatment?
[HJH 2022-01-10: Some minor formatting and grammar issues were bugging me, so I corrected them.]