A human embryo at the 4th week of development is just a tiny bean with a length measured in millimeters, but at this time all kinds of remarkable features are starting to develop. This week in class I talked about urogenital development, which involves forming an array of incredibly delicate, thin tubes from a structure called the urogenital ridge, a thickening of an embryonic membrane which will eventually form a succession of kidneys, the pronephros, mesonephros, and metanephros, only the last persisting into adulthood. The key feature for the story I was telling, though, is that they formed something called the mesonephric duct, and then the paramesonephric duct which parallels it. Another name for the mesonephric duct is the Wolffian duct, and the paramesonephric duct is called the Müllerian duct (personally, I don’t care for the self-serving names given to critical bits of the developing embryo by 19th century men, but it’s what still persists in the embryo. So it goes.)
Both of these ducts are associated with the bipotential or indifferent gonad. There are no sexual differences in embryos this young.

The sex differences emerge later, in response to differential signals. The Müllerian ducts degenerate in males, while the Wolffian ducts persist. In females, the Müllerian ducts persist, while the Wolffian ducts fade away. The bipotential gonad associates with the remaining duct and differentiates into testes or ovaries.

I’ll refrain from delving deeper into the details. My point is that these minuscule ducts and tissues form very early, and are going to expand to form critical, elaborate structures necessary for human fertility. They’re fragile. You really don’t want to perturb the signals and processes going on in a one month old embryo, especially since you may not see the consequences for 15 or 20 years.

In 1941, pharmaceutical companies started to market a synthetic drug with properties similar to estrogen, called diethylstilbesterol, or DES. It wasn’t patented, so anyone could make and sell it, and they pushed it hard to pregnant women. There was weak evidence that it could help sustain pregnancies in women with low progesterone levels, so sure, let’s market it as “routine prophylaxis in ALL pregnancies.” About 4 million pregnant women took this stuff at the suggestion of their doctors, between 1941 and 1971, when it was finally banned.
Think about that. This was an endocrine disruptor, term that wasn’t invented until the 1990s, but everyone knew then that it would have some kind of effect, since it was a functional analog of estrogen. So they gave it to pregnant women, and by that means delivered a potent hormonal signal to their embryos at a time when they were carefully assembling those delicate little tubes. Worse, they knew that high doses given to mice and hamsters caused mammary, cervical, vaginal, and uterine cancers in adult females, and that adult males developed lung cancers, which ought to have set off all kinds of alarm bells. Any tissue that was sensitive to estrogen could be provoked to turn cancerous with DES.
Just for dessert, it was determined in 1953 that DES did nothing to maintain at risk pregnancies. They continued to prescribe the stuff. Just in case, you know.
For additional profit, they also marketed it as a growth hormone for livestock. That continued until it was eventually banned for that purpose in 1979.
Here’s the structure of this potent little molecule.

A is DES; B is estrogen; C is BPA, the common, heavily used plasticizer that we now know is an endocrine disruptor.
You might be wondering what happened to those 4 million women who took the drug. They were fine! Humans and other primates seem to be more resistant to the carcinogenic effects of DES, and they were taking much lower doses than those poor rodents in testing labs who were given massive doses of the drug.
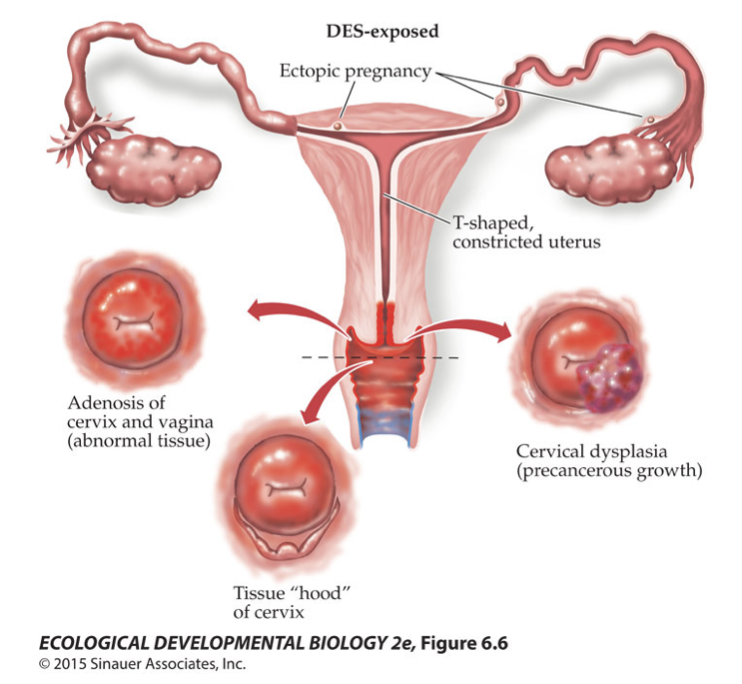
And what about the millions of boomer babies who were doped with it in utero? Again, mostly fine — this is the thing about endocrine disruptors, they tend not to have the gross teratogenic effects we associate with chemicals that cause significant birth defects, like thalidomide. They’re more subtle. They perturb the balance of internal organ systems, and in this case, cause problems in the physiology of reproductive organs, which may lead to fertility issues or some kinds of cancers. I emphasize may because I know DES-exposed people who have had children and are cancer-free; it’s more a matter of letting their gynecologists know to keep an eye on potential warning signs.
But it can go very wrong.
DES is still used in experimental studies because it’s such an interesting molecule. Regular readers probably know about the importance of Hox genes; these are genes expressed along the body axis in pretty much all animals that defined anterior-posterior structures. The same genes also get re-expressed to define the proximal-distal axis of the tetrapod limb. They seem to be a handy-dandy molecular tool for establishing tissue identities along a line.
Here’s another instance of Hox genes defining position on an organ: they’re re-expressed in the Müllerian ducts, which become the fallopian tubes of adult women.
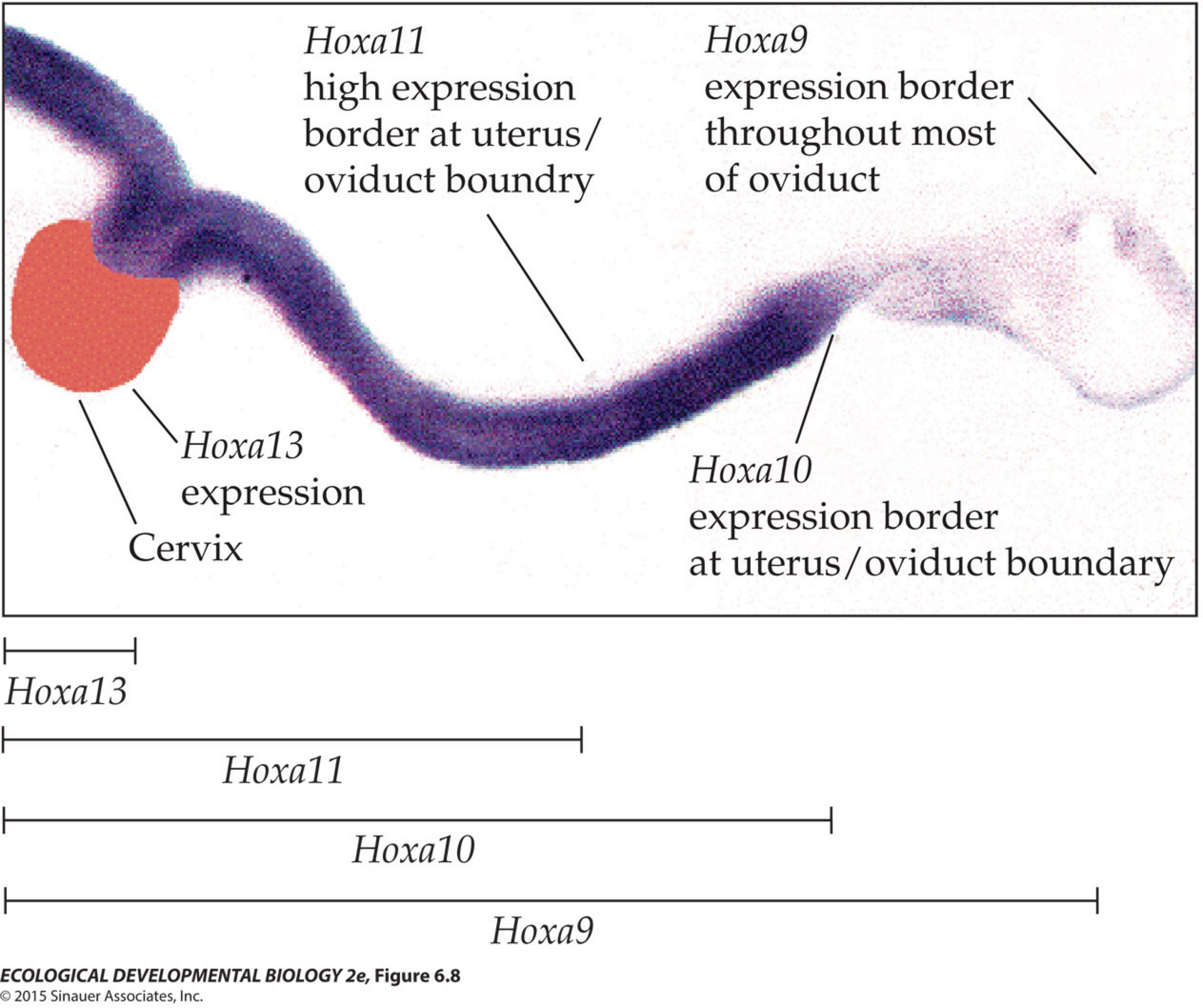
Hoxa9 is expressed throughout the oviduct, Hoxa13 in only the cervix, and Hoxa11 and Hoxa10 in between, forming a kind of positional coding system. This is really neat! I like finding examples of molecular recycling in the evolution of developing systems.
What isn’t so neat is that DES downregulates Hoxa10 by inhibiting an important signaling molecule, Wnt7a, creating coding ambiguities in the structure of that delicate little tube. That leads to poor cell specification and disorganized tissue, erasing what should be clear, sharp boundaries in the organ, which may then be expressed in dysplasias, increasing the odds of cancer.
As if that weren’t enough, we don’t really know what perturbing these signaling pathways does to other developing organs, like the brain. Also, DES affects methylation/demethylation of the genome, so it may have transgenerational effects — pregnant women who took DES may have messed up their children, but there is some evidence (weak, I think) that it also affects their grandchildren.
But wait! It’s banned, so we shouldn’t have to worry about it anymore! That’s partly true, but look at the diagram of the molecules above. Estrogen and DES share similarities to another molecule, bisphenol A, a ubiquitous plasticizer used to make plastic materials less brittle. BPA is found in your food packaging. It lines the interior of aluminum cans. Any plastic you have that is at all flexible has been treated with plasticizers, like BPA or phthalates. It’s leaching into your food and your general environment, and it does not go away. The US has banned its use in baby bottles and baby formula packaging, but not from all your snack food packages and your phones.
If you’re of a certain age, you might recall those commercials for a dishwashing detergent that announced, “you’re soaking in it!“, as if that meant the stuff must be safe. We ought to be aware that capitalist industries have us all soaking in a gentle bath of toxic chemicals right now, and it’s not safe.